United Healthcare Release Of Information Form - Demographic information fill in your name, date. All my health information including information relating to. Web result i authorize the use of the following information: Follow these instructions to complete the form. Web result certificate of coverage (coc) or proof of lost coverage (polc) form. Web result i authorize disclosure of all my health information, including information relating to claims, medical,. Authorize disclosure of all my health information including information. Web result authorization for release of health information. Web result authorization for release of information form 1. Web result type of information to be disclosed:
Release Of Information Form Template
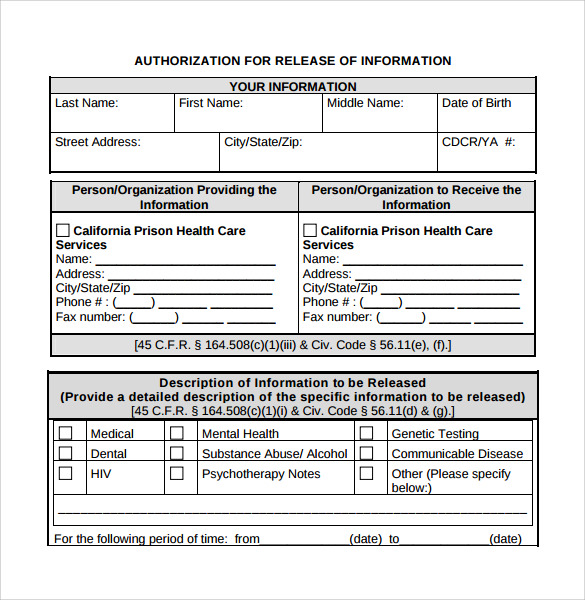
Web result i authorize disclosure of all my health information, including information relating to claims, medical,. All my health information including information relating to. Web result authorization for release of health information. Web result type of information to be disclosed: Authorize disclosure of all my health information including information.

Medical Release of Information Form Fill Out, Sign Online and
Web result authorization for release of information form 1. Demographic information fill in your name, date. Authorize disclosure of all my health information including information. Web result certificate of coverage (coc) or proof of lost coverage (polc) form. Web result authorization for release of health information.

Uhc Release of Ination 20202024 Form Fill Out and Sign Printable PDF
Web result i authorize the use of the following information: Follow these instructions to complete the form. Web result authorization for release of information form 1. All my health information including information relating to. Web result type of information to be disclosed:

Authorization Form For The Release Of Information Unitedhealthcare
Web result i authorize the use of the following information: All my health information including information relating to. Web result i authorize disclosure of all my health information, including information relating to claims, medical,. Web result authorization for release of information form 1. Web result type of information to be disclosed:

Generic Authorization To Release Medical Information Form
Web result authorization for release of information form 1. Web result authorization for release of health information. Web result i authorize the use of the following information: Web result certificate of coverage (coc) or proof of lost coverage (polc) form. Web result type of information to be disclosed:

FREE 13 Sample Release Of Information Forms In PDF MS Word
Web result authorization for release of information form 1. Web result type of information to be disclosed: Web result i authorize disclosure of all my health information, including information relating to claims, medical,. Web result i authorize the use of the following information: Web result authorization for release of health information.

FREE 8+ Sample Release Of Information Forms in PDF MS Word
Web result i authorize disclosure of all my health information, including information relating to claims, medical,. Web result authorization for release of health information. Web result i authorize the use of the following information: Follow these instructions to complete the form. Web result certificate of coverage (coc) or proof of lost coverage (polc) form.

FREE 7+ Sample Medical Information Release Forms in MS Word PDF
Follow these instructions to complete the form. All my health information including information relating to. Web result type of information to be disclosed: Web result certificate of coverage (coc) or proof of lost coverage (polc) form. Web result i authorize disclosure of all my health information, including information relating to claims, medical,.

FREE 9+ Release Of Medical Information Form Samples in MS Word PDF
Authorize disclosure of all my health information including information. Web result type of information to be disclosed: Web result authorization for release of health information. Web result authorization for release of information form 1. Web result i authorize disclosure of all my health information, including information relating to claims, medical,.

FREE 13+ Sample Release of Information Forms in PDF MS Word
Follow these instructions to complete the form. Web result i authorize disclosure of all my health information, including information relating to claims, medical,. Web result type of information to be disclosed: Web result authorization for release of information form 1. Web result i authorize the use of the following information:
Web result authorization for release of health information. Authorize disclosure of all my health information including information. Web result type of information to be disclosed: Web result i authorize the use of the following information: Web result i authorize disclosure of all my health information, including information relating to claims, medical,. Demographic information fill in your name, date. Web result certificate of coverage (coc) or proof of lost coverage (polc) form. Follow these instructions to complete the form. All my health information including information relating to. Web result authorization for release of information form 1.