Texas First Report Of Injury Form - Name (last, first, m.i.) 2. Send the specified copies to your workers' compensation insurance carrier and the. 10/05) page 3 division of workers’ compensation. Web employers first report of injury or illness. Web employers first report of injury or illness.

First Report Of Injury/illness Form printable pdf download
Web employers first report of injury or illness. Send the specified copies to your workers' compensation insurance carrier and the. Web employers first report of injury or illness. 10/05) page 3 division of workers’ compensation. Name (last, first, m.i.) 2.

Fillable First Report Of Injury printable pdf download
Send the specified copies to your workers' compensation insurance carrier and the. Name (last, first, m.i.) 2. 10/05) page 3 division of workers’ compensation. Web employers first report of injury or illness. Web employers first report of injury or illness.

First Report of injury/Notification Letter
Web employers first report of injury or illness. Name (last, first, m.i.) 2. 10/05) page 3 division of workers’ compensation. Send the specified copies to your workers' compensation insurance carrier and the. Web employers first report of injury or illness.
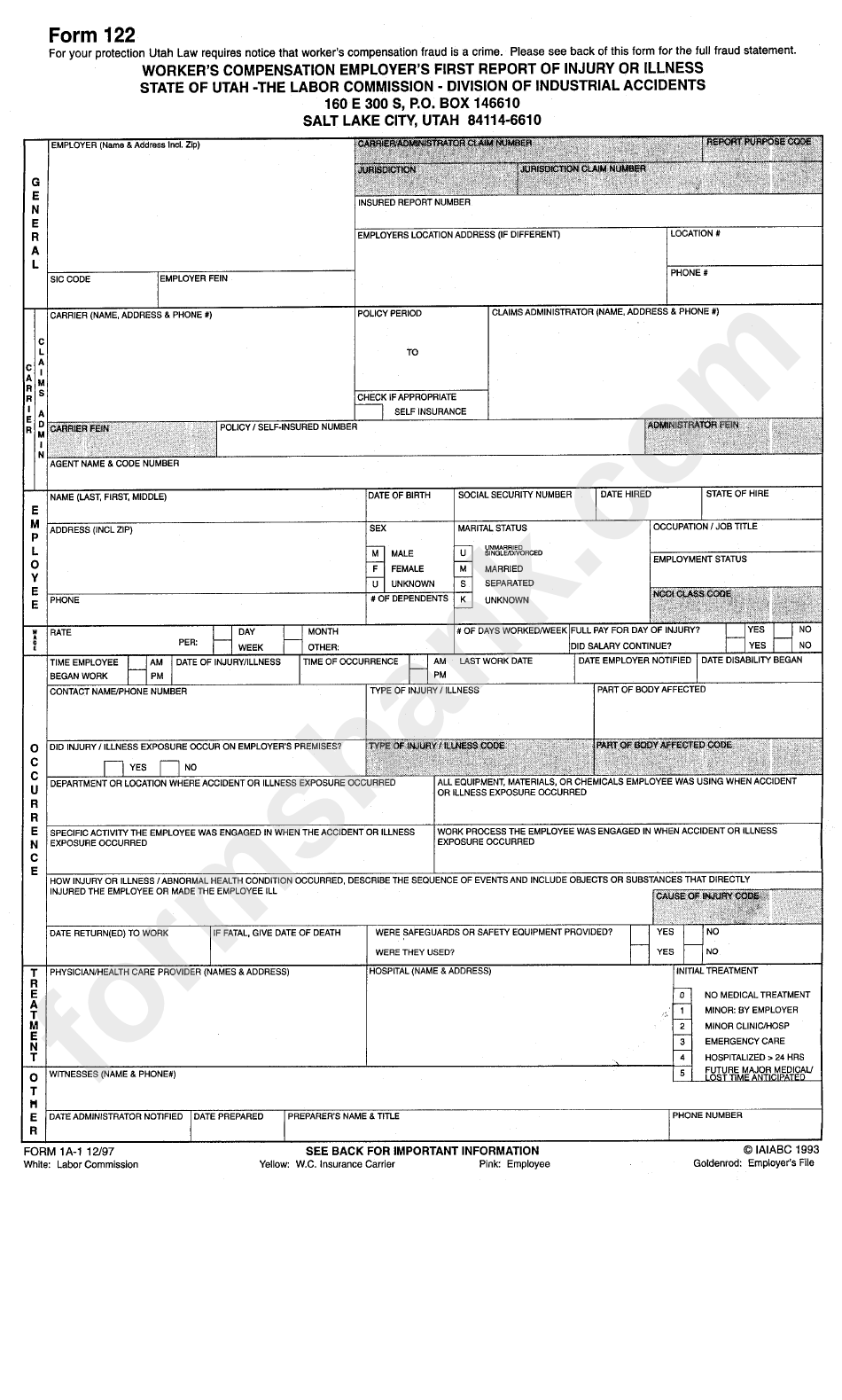
Form 122 Workers Compensation Employers First Report Of Injury Or
10/05) page 3 division of workers’ compensation. Send the specified copies to your workers' compensation insurance carrier and the. Web employers first report of injury or illness. Name (last, first, m.i.) 2. Web employers first report of injury or illness.

Top 18 First Report Of Injury Form Templates free to download in PDF format
Web employers first report of injury or illness. Web employers first report of injury or illness. 10/05) page 3 division of workers’ compensation. Send the specified copies to your workers' compensation insurance carrier and the. Name (last, first, m.i.) 2.

WC1 EMPLOYERS FIRST REPORT OF INJURY OR OCCUPATIONAL Fill and
Web employers first report of injury or illness. Name (last, first, m.i.) 2. Web employers first report of injury or illness. Send the specified copies to your workers' compensation insurance carrier and the. 10/05) page 3 division of workers’ compensation.

Tx Workers Form Fill Out and Sign Printable PDF Template SignNow
Name (last, first, m.i.) 2. 10/05) page 3 division of workers’ compensation. Send the specified copies to your workers' compensation insurance carrier and the. Web employers first report of injury or illness. Web employers first report of injury or illness.

First Report Of Injury Form Fill Out and Sign Printable PDF Template
10/05) page 3 division of workers’ compensation. Send the specified copies to your workers' compensation insurance carrier and the. Web employers first report of injury or illness. Name (last, first, m.i.) 2. Web employers first report of injury or illness.

Harris Texas First Report of Injury for Workers' Compensation US
Send the specified copies to your workers' compensation insurance carrier and the. 10/05) page 3 division of workers’ compensation. Web employers first report of injury or illness. Name (last, first, m.i.) 2. Web employers first report of injury or illness.

Form DWC1S Fill Out, Sign Online and Download Fillable PDF, Texas
Web employers first report of injury or illness. 10/05) page 3 division of workers’ compensation. Web employers first report of injury or illness. Send the specified copies to your workers' compensation insurance carrier and the. Name (last, first, m.i.) 2.
Send the specified copies to your workers' compensation insurance carrier and the. Web employers first report of injury or illness. Web employers first report of injury or illness. 10/05) page 3 division of workers’ compensation. Name (last, first, m.i.) 2.